


BLOG
Which ACL Graft Is Best? A Performance Therapist's Guide for Athletes
Short answer: There isn't one "best" ACL graft for every athlete. The ideal graft depends on your sport, position, age, previous injuries, and the demands you'll place on your knee after surgery. In this article we'll compare the three most common graft options—quadriceps tendon, patellar tendon, and hamstring tendon—from a rehabilitation and return-to-sport perspective.
Jul. 11, 2026
Dr. Donald Mull, DC

Short answer: There isn't one "best" ACL graft for every athlete. The ideal graft depends on your sport, position, age, previous injuries, and the demands you'll place on your knee after surgery. In this article we'll compare the three most common graft options—quadriceps tendon, patellar tendon, and hamstring tendon—from a rehabilitation and return-to-sport perspective.
ACL tears have been an increasingly common topic and rightfully so as ACL tear rates have continued to rise especially in youth sports (young female athletes being the most affected).(1)
One hard cut. One that has been done thousands of times, but this time the knee buckles and there is a loud pop. Everyone holds their breath as the athlete winces in pain grabbing their knee. Some can walk off with a slight limp and others need to be helped to the sideline.
What to do next can be overwhelming. How do you know if you tore an ACL? Where do we go from here? Do we go to the ER? If you're lucky enough to have an athletic trainer present, are they able to definitively say what just happened?

An ACL injury oftentimes cannot be ruled out even if the knee "feels" stable with on-field assessments. Muscles can guard so tightly that it gives an illusion of ligament stability. Therefore when an athlete feels a pop accompanied with a knee injury an MRI is considered the gold standard to rule out an ACL injury. It is normally (but not always) accompanied with swelling, buckling/giving out and/or inability to walk or comfortably bear weight.
It is best to consult with an orthopedic surgeon as soon as possible to receive an MRI as well as discuss what the best options are moving forward. A big question once an ACL injury has been confirmed is what ACL graft one should get. As I am not an orthopedic surgeon, I am not the best resource to give advice on which is best from a surgical standpoint so I will focus mainly on the rehab and return to play perspective.
What I can say is that the individual goals, which sports the athlete plays as well as which position the athlete plays should be taken into consideration.
The most common grafts that are used are hamstring tendon, quadricep tendon and bone-patellar-bone grafts. Each of these grafts come with considerations.
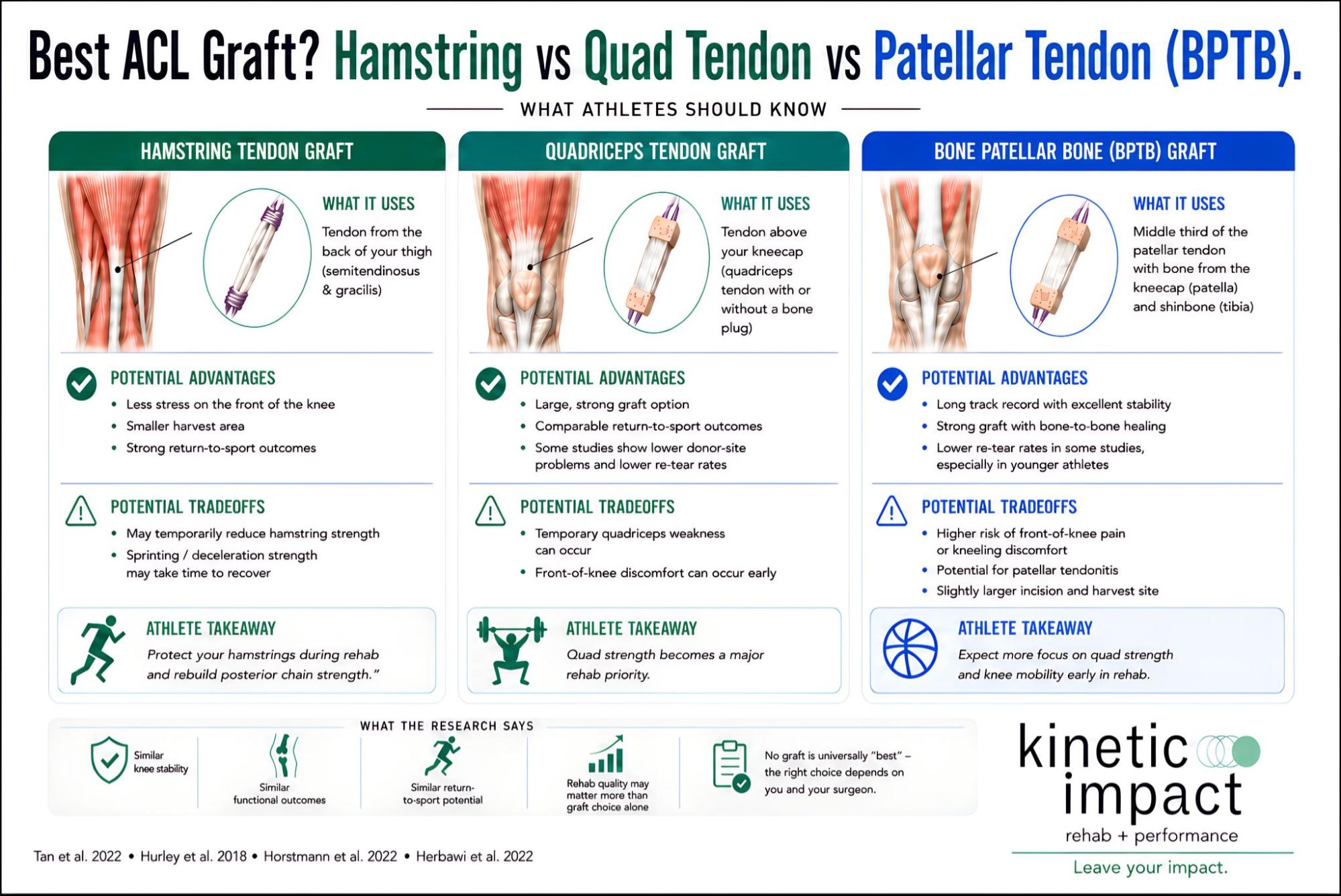
Figure 1. Comparison of the three most common ACL graft options—hamstring tendon, quadriceps tendon, and bone-patellar tendon-bone (BPTB)—including rehabilitation considerations, advantages, and tradeoffs for athletes returning to sport.
| Feature | Hamstring | Quad Tendon | Patellar Tendon(BPTB) |
|---|---|---|---|
| Re-tear risk | Slightly higher in some studies | Very low | Very low |
| Anterior knee pain | Lowest | Moderate | Highest |
| Sprinting considerations | Hamstring strength recovery is important | Minimal | Minimal |
| Jumping/Cutting | Good | Quad strength is a major focus | Quad strength is a major focus |
| Early rehab | Often progresses slightly faster | May have more anterior knee symptoms | May have more anterior knee symptoms |
| Best for | Some athletes depending on sport | Excellent all-around option | Excellent option for many cutting/pivoting athletes |
Because of how closely related the harvest sites are, the quad tendon and bone-patellar-bone grafts have a lot of similar considerations when it comes to rehab and recovery from surgery.
The quadriceps and bone-patellar-bone grafts have been shown to have the least amount of risk for retear rates(2), though the difference is quite small and not consistent amongst all evidence.(3,4) One important side note here is the risk of retearing the ACL on the same knee or opposite knee is significantly higher in athletes younger than 18 years old.(5)
A consideration for both quadriceps tendon and bone-patellar-bone grafts are the association with front of the knee pain during the rehab and return to play process (which makes sense since a chunk of the quad or patellar tendon is taken to help remake the ACL). So there should be a large focus on building quad strength as early and often as possible to help mitigate as much as this as possible, especially when demands increase throughout the rehab process.
When it comes to mobility, both quad and patellar grafts may need some extra work likely due to the strength of the grafts themselves. So if your sport requires a lot of deep knee flexion like wrestling or libero in volleyball then it may take longer to feel comfortable forcefully flexing the knee in deeper angles. This should direct the rehab to focus on restoring range of motion as quickly as possible, spending more time and effort to ensure lack of mobility does not negatively affect running and cutting biomechanics.
The recovery and progression experienced during rehab of hamstring grafts have been reported to be slightly faster than the quadriceps grafts(6), though again very marginal differences. This is likely due to less anterior knee pain that can be associated with quad or patellar grafts. Also, the best evidence does NOT support using timeline alone to determine return to play but rather using readiness or physical capabilities. This makes sense because time doesn't prepare you for a sport, your abilities and confidence does. This means when someone tells you in 9 months you will be playing again - this is very bad advice.
This means diligently testing the knee's strength, jump abilities, cutting and sprinting quality as well as gradual return to drilling, non contact then contact sport participation before deeming ready to return to full participation. Those who meet the standards of physical capabilities are more likely to be healthy and play at pre-injury levels for longer (and this is the whole point right?).(7)
As the athlete moves to later stages of rehab where sprinting, jumping and cutting becomes much more important to train, other considerations must be taken into account.
When it comes to jumping and cutting the athlete needs to be able to decelerate, which is a very demanding task for the knee, the quadriceps muscle group in particular.(8) Thus when an athlete has a quad graft it is very important that the strength of the quad has been trained to not only be strong but to also be able to contract extremely fast. It is not uncommon for those who have had a quad or patellar graft to experience pain in the front of the knee as they are exposed to jumping and cutting.
As for sprinting and slowing down from sprinting, the hamstrings experience extremely high forces.(9) These forces exceed what can be done in the weightroom so complications can present themselves once the athlete starts getting closer to speeds they will experience in sport. In addition to a very heavy quad strength and power focus, attention should be paid to the hamstring group to ensure that a foundation of strength and power is laid out in addition to progressively exposing the athlete to a variety of sprint drills.
At the end of the day, the goals and type of athlete should be openly discussed with the surgeon so they have the entire context and can give their best opinion based on the individual athlete. As for the rehab process, the graft should help aid the clinician's decision making as well as education during the rehab process. This is not a one size fits all scenario and the athlete should be treated as an individual.
Whichever graft is chosen for the athlete, remember that time alone does not prepare the athlete to play their sport at a high level again. The best way to ensure your athlete safely returns to sport is to make sure you have a rehab provider that will teach the athlete how to achieve the necessary capabilities needed in their sport. Time does not dictate whether they are ready to go back, their physical abilities and confidence do.
Sources
Graphic Sources
Related Posts
Chiropractic vs Physical Therapy: What is the Difference?
However we want to dispel this misconception once and for all. We sat down and talked about it. You may be surprised by the c...
Read more
4 Ways to Quickly Relieve Tight Muscles (including detailed video examples)
In a previous blog Why Do Muscles Feel Tight, we talked about why your muscles get tight. Now we have a sense of what may be ...
Read more
Ditch the Situps: Your Back will Thank You
By now most of us know that effective core training is essential for staying active and pain free. In an effort to build stre...
Read more
Search the Blog




